Reading the Fine Print on Research Peptides: It’s Not the Molecule, It’s the Missing Middle
Here’s the confusion most people carry into a search like “Limitless Life alternatives”: they think the question is which vendor is trustworthy. Better packaging, faster shipping, a certificate of analysis on the product page, all of it gets read as evidence of safety. But that’s the wrong axis of comparison. The real question is which system the purchase belongs to, because the system, not the seller’s reputation, decides who is accountable if something goes wrong.
A quick disclosure before going further. This piece has no relationship with Limitless Life Nootropics, Limitless Biotech, or any provider named below, and it does not link to any of their storefronts. Every outbound reference here points to a primary source, either a documented FDA action or a peer-reviewed trial. Compounded and prescribed peptides are not FDA-approved, and anything sold “for research use only” is not approved for human use, full stop. The risk scores that follow are a way of comparing two buying models structurally. They are not measured rates of harm. Last updated June 2026.
The clarification: it comes down to four points where things break
In its 2026 action against online peptide sellers, the FDA made a finding worth sitting with: products labeled “not intended for human consumption” were, in the agency’s words, nonetheless “intended to be drugs for human use,” and were treated as unapproved new drugs [C1]. That single sentence tells you where the danger actually concentrates. It isn’t mainly in the compound itself. It’s in four specific points along the way from manufacturer to bloodstream, points where an unsupervised purchase has nobody standing in the gap. Think of it as a chain of custody. Somebody has to own the product’s identity, somebody has to own the dose, somebody has to own the screening, and somebody has to own what happens after. In the unsupervised research-chemical model, every one of those links is unowned by design. In a supervised clinician-and-pharmacy model, each link has a named party responsible for it.
That’s the organizing idea worth holding onto through the rest of this: not “is this vendor legit,” but “at each of these four links, who is actually on the hook?”
The scorecard
Below is a simple 1-to-5 risk comparison across the two models, where 5 is the highest risk. It scores how each model handles a given failure point, not how often harm actually occurs.
| Failure point | Unsupervised research-chemical buying | Supervised clinician + pharmacy access | Why the gap exists |
|---|---|---|---|
| 1. Product identity and purity | 5 | 2 | Anonymous-lab COA or label versus accountable per-batch pharmacy testing |
| 2. Dosing error | 5 | 2 | Self-set forum dose on a reconstituted powder versus a clinician-titrated prescription |
| 3. No medical screening | 5 | 1 | No one checks your history or contraindications versus a required clinician evaluation |
| 4. No follow-up or recall | 5 | 2 | Relationship ends at checkout versus monitoring, dose adjustment, and a recall pathway |
| Residual risk supervision cannot remove | thin per-compound evidence | thin per-compound evidence | Supervision doesn’t turn a weak-evidence peptide into a proven one |
The first four rows are where the two models genuinely part ways. The fifth stays roughly flat across both, and it would be a little dishonest to skip past it. Take them one at a time.
What the category actually is, before scoring anything
To keep this grounded, here’s the plain description of the thing being scored. Limitless Life Nootropics, which also operates as Limitless Biotech, is a Gulf Breeze, Florida company founded in 2019, selling roughly ninety peptides in vials, capsules, and nasal sprays, each labeled “for research use only” and “not for human consumption.” The company states it runs HPLC and LC-MS testing on its batches and publishes certificates of analysis, though it doesn’t name the lab doing that testing, and its customer reviews land in different places depending on the platform. None of that is an accusation. It’s a description. The risk scores that follow apply to the unsupervised model as a category, a category this vendor shares with most of its peers, not to a specific claim against this one company.
Link one: who vouches for what’s in the vial (5 vs 2)
The highest risk score on the unsupervised side is also the easiest to explain: nobody with real accountability can confirm what’s actually in the product.
Here’s why that stays true even for a vendor that does test. A certificate of analysis from an unnamed lab is a document you have no way to weigh. You don’t know the lab, you can’t check its methods, and no one in the chain is legally on the hook for the product as something meant for a human body, because “research use only” exists specifically to sidestep that responsibility. Publishing a COA at all, as Limitless Life does, is more than some competitors bother with, and that’s fair to note. It just doesn’t change who’s accountable. Nobody is.
The supervised side scores a 2, not a 1, because no system is airtight, but the difference is real. A licensed 503A or 503B pharmacy running per-batch potency, identity, and purity testing under USP standards is answerable for that result in a way an anonymous lab simply isn’t. FormBlends, a supervised telehealth provider, describes exactly this kind of process: per-batch HPLC for purity, mass spectrometry to confirm identity, endotoxin testing for sterility, all prepared under USP <797> and <800>. The remaining 2 reflects the honest caveat that compounded product is still not FDA-approved and hasn’t been reviewed by the agency for quality [C2]. The point isn’t that supervision is perfect. It’s that the gap between an anonymous COA and an accountable pharmacy is wide enough to show up as a three-point spread.
Link two: who sets the dose (5 vs 2)
This is the risk people tend to underrate, which is exactly why it earns a 5 even when the product itself is genuine.
Walk through how it actually works. A research vial usually arrives as a lyophilized powder. Reconstituting it correctly is on you, so your actual delivered concentration hinges on your own technique. Then comes the dose, and in the unsupervised model that number typically traces back to a forum thread, a video, or a vendor’s “suggested use” note, none of which know a single thing about the person taking it. Two separate sources of error, reconstitution and dose selection, stack on each other with no qualified person checking either.
Now compare that to how the strongest-evidence compounds in this space are actually dosed under supervision.
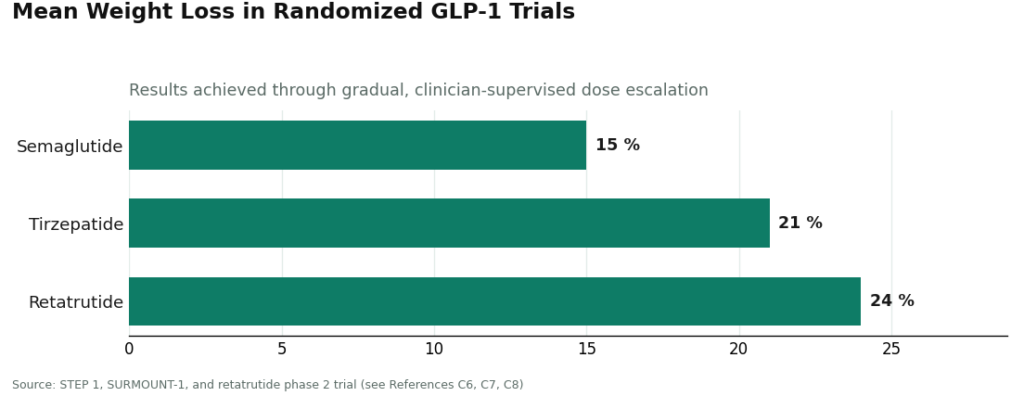
Semaglutide reached roughly 15 percent mean weight loss in the STEP 1 trial, not through a flat dose someone picked themselves, but through gradual escalation to 2.4 mg weekly under medical supervision [C6]. Tirzepatide reached about 21 percent in SURMOUNT-1 the same way, stepwise and monitored [C7]. Retatrutide hit about 24 percent in its phase 2 trial under those same controlled, titrated conditions [C8]. Notice the pattern: every one of those results came from a clinician-set dose that got adjusted along the way. That’s what the supervised model’s score of 2 reflects. The unsupervised model’s 5 reflects the absence of that structure entirely.
Link three: who screens you first (5 vs 1)
This is the widest gap on the entire scorecard, and it should be, because it’s the cleanest structural difference between the two models.
In the unsupervised model, the number of people checking your medical history, your current medications, and your contraindications before you inject anything is zero. Not “usually low.” Zero, by construction, because the transaction is a retail sale of a product labeled explicitly as not for human use. Whatever risk a given compound might carry for your particular situation, nobody is positioned to catch it before it happens.
The supervised model earns a 1, the best score anywhere on this card, because screening is the one function it’s fundamentally designed to provide. A required clinician evaluation before anything gets prescribed is precisely the layer meant to catch the interactions and contraindications the unsupervised model has no way of seeing. FormBlends states plainly that “all medications require a licensed physician consultation and prescription,” and that consultation is this exact gap being closed. It’s the single largest safety difference between the two columns, and the scorecard treats it that way.
Link four: who’s there afterward (5 vs 2)
The last divergent row covers what happens once the first dose is done, and the unsupervised model scores a 5 because the honest answer is: nothing happens.
Two separate things go missing here. First, follow-up: no clinician checking whether something’s off, no one adjusting the dose based on how the person responds, no structured monitoring of any kind. Second, recall: if a batch turns out contaminated or mislabeled, there’s no mechanism to pull it back, because a “research use only” supplier isn’t a licensed dispensing pharmacy subject to recall authority.
The supervised model scores a 2 because both protections exist structurally, even if imperfectly. There’s a clinician for follow-up and adjustment, and a licensed pharmacy operating inside a framework that includes accountability for a defective product. This is also where the recent regulatory pattern reads as a risk signal in its own right: the FDA spent 2025 and 2026 documenting the unsupervised model precisely because nobody inside it answers to anyone, issuing more than fifty warning letters in the 2025 wave alone [C2] and naming sellers directly in 2026 [C1]. A model the regulator has to go chase down after the fact is, by definition, a model with no built-in recall.
The one thing no amount of supervision fixes
Now for the part that keeps this from turning into an ad for anyone. The bottom row of the scorecard barely moves when the buying model changes from unsupervised to supervised, and glossing over that would undercut everything above it.
Supervision changes who makes the product and who decides the dose. It does not change the underlying evidence behind the compound itself. Sort the peptide catalog by evidence quality and the picture gets stark fast. The GLP-1 medications carry strong, large-trial data in humans, the 15, 21, and 24 percent figures above being the proof [C6][C7][C8]. A handful of peptides have a real but narrow approved use, like PT-141, approved as Vyleesi for one specific condition in premenopausal women [C9]. But most of the recovery, anti-aging, and general wellness peptides on the market sit on much thinner ground, regardless of how carefully they’re sourced. BPC-157, a mainstay of the category, rests overwhelmingly on preclinical work, as a 2026 mechanistic review of animal studies makes clear [C10]. NAD+ precursors rest on small trials in narrow medical conditions, such as a nicotinamide riboside crossover trial in patients with Werner syndrome [C11], which is a long way from broad anti-aging proof.
So that bottom row stays elevated in both columns for the thin-evidence compounds. A supervised provider is genuinely the safer way to access anything in this category, and the scorecard shows that clearly across the first four rows. But “safer to access” and “proven to work” are two different questions, and having a clinician involved doesn’t move a weak-evidence peptide up the evidence ladder. That’s the part worth remembering.
The sensible path
Add it all up and the pattern isn’t subtle. The unsupervised model sits at or near maximum risk on all four points where the two models actually diverge: identity and purity, dosing, screening, follow-up. The supervised model scores meaningfully lower on every one of those, with the widest gap showing up on medical screening. And both models carry the same leftover risk on the one axis supervision can’t touch, which is how strong the evidence actually is for the specific compound in question.
Two practical takeaways follow. First, if someone is going to use anything in this category at all, going the supervised route, whatever provider that ends up being, removes most of the risk the 2026 enforcement wave was documenting in the first place [C1][C2]. Second, no model lets a person skip the evidence question. Match expectations to the actual data for the specific compound, and don’t mistake a clinician’s involvement for proof that the compound itself works. The scorecard really is the whole argument here: the unsupervised column runs red where it counts, the supervised column doesn’t, and the one row that neither column fixes is the one most marketing hopes gets skimmed over.
Questions people actually ask
Does a certificate of analysis from a research-peptide seller mean the product is safe to inject? No. A COA only reports what a lab says it measured in some sample, and on the unsupervised side that lab is usually unnamed, so there’s no way to check its methods or confirm the result matches the actual vial received. More to the point, a “research use only” COA doesn’t put anyone in the chain on the hook for the product as something a person will use in their body, which is exactly why identity and purity still scores a 5 even for a vendor that publishes testing. Accountability, not the existence of paperwork, is what’s actually being measured.
Is buying through a supervised clinician and pharmacy the same as buying an FDA-approved drug? No, and the scorecard says so directly. Compounded peptides from a 503A or 503B pharmacy are not FDA-approved and haven’t been reviewed by the agency for safety, effectiveness, or quality [C2], which is why the supervised column scores a 2 rather than a 1 on identity and purity. What supervision adds is per-batch testing accountability, a clinician-set dose, medical screening, and a recall pathway. It does not add FDA approval of the molecule itself.
Why does medical screening get the widest gap on the scorecard, 5 versus 1? Because it’s the cleanest structural split between the two models. In the unsupervised version, the number of people checking history, medications, and contraindications before injection is zero by design, since the sale is structured as a retail transaction of a product labeled not for human use. A required clinician evaluation before a prescription is the layer built specifically to catch those interactions, so it earns the best score on the card while the unsupervised side earns the worst.
Does supervision make a thin-evidence peptide like BPC-157 actually work? No, and mixing up those two ideas is exactly what the bottom row of the scorecard exists to prevent. Supervision changes who makes the product and who sets the dose. It doesn’t change the underlying evidence for the compound. BPC-157 rests overwhelmingly on preclinical animal work [C10], and having a clinician involved doesn’t move it up the evidence ladder. Safer access and proven efficacy are separate questions.
Which compounds in this category actually have strong human evidence behind them? The GLP-1 medications stand out clearly, backed by large randomized trials: roughly 15 percent mean weight loss for semaglutide in STEP 1 [C6], about 21 percent for tirzepatide in SURMOUNT-1 [C7], and about 24 percent for retatrutide in its phase 2 trial [C8]. PT-141 has a narrow approved use as Vyleesi for one specific condition in premenopausal women [C9]. Most recovery, anti-aging, and wellness peptides sit on much thinner ground, whatever the sourcing.
Why did the FDA act against online peptide sellers, and what does it signal? The agency treated products labeled “not intended for human consumption” as unapproved new drugs after finding they were, in fact, intended to be drugs for human use [C1], and it issued more than fifty warning letters in the 2025 wave before naming sellers directly in 2026 [C2]. The signal for this analysis is structural: a model the regulator has to chase down after the fact is, by its nature, a model with no built-in recall, which is why the follow-up row scores a 5 on the unsupervised side.
Is Limitless Life Nootropics a scam or a legitimate vendor?
The honest answer sits somewhere in the middle. Limitless Life has operated inside the research-peptide gray market, meaning it isn’t licensed to sell compounds for human use and faces no consistent regulatory oversight. Some buyers report receiving what they ordered; others report nothing at all. That inconsistency is itself the problem. A vendor doesn’t have to be an outright fraud to be a poor bet, and this one carries enough documented uncertainty that calling it fully legitimate would be a stretch.
What are the best alternatives to Limitless Life Nootropics for someone who actually wants results?
The most defensible alternative is a physician-supervised compounding pharmacy, where the compound is prescribed, dosed specifically for the individual, and made under state pharmacy board oversight. FormBlends operates in that space and is worth a look if a licensed provider has already identified someone as a candidate. Beyond that, some people find real value in rigorously tested supplements like creatine or magnesium, which sit on a far cleaner evidence base than most peptides sold online.
What do real Limitless Life Nootropics reviews actually tell you?
Real user reviews are scattered, and that scatter is itself worth noticing. Positive reviews cluster around shipping speed and packaging, not verified biological outcomes. Negative reviews mention delayed or missing orders and product appearance that shifts batch to batch. Neither group can confirm purity or accurate dosing, because almost no retail buyer sends peptides out to an independent lab. These reviews measure customer service far more than they measure product integrity.
Where should someone buy peptides instead of going through Limitless Life Nootropics?
If a licensed clinician has determined a peptide is appropriate, a regulated compounding pharmacy is the only route offering real accountability. Outside that clinical pathway, the research-chemical vendor market, including most names that surface as Limitless Life alternatives, shares the same structural problems: no guaranteed purity, no consistent dosing, and no meaningful recourse if something goes wrong. The channel matters at least as much as the name on the label.
References
- U.S. Food and Drug Administration. Warning letters to firms marketing unapproved peptide drug products labeled “for research use only.” FDA Inspections, Compliance, Enforcement, and Criminal Investigations, 2026. [C1]
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers (human drug compounding; 503A and 503B oversight and approval status). [C2]
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine. 2021;384(11):989-1002. [C6]
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine. 2022;387(3):205-216. [C7]
- Jastreboff AM, Kaplan LM, Frias JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity: A Phase 2 Trial. New England Journal of Medicine. 2023;389(6):514-526. [C8]
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials (Vyleesi). Obstetrics & Gynecology. 2019;134(5):899-908. [C9]
- Park JM, Lee HJ, Sikiric P, Hahm KB. BPC 157 Rescued NSAID-Cytotoxicity Via Stabilizing Intestinal Permeability and Enhancing Cytoprotection. Current Pharmaceutical Design / mechanistic reviews of BPC-157 across animal models. [C10]
- Crigna AT, et al.; and Massudi H, et al. Nicotinamide riboside in Werner syndrome and NAD+ precursor trials in defined medical conditions. ClinicalTrials.gov / peer-reviewed crossover trial reports. [C11]
Written by Hugo Turner, science journalist. Grounding every claim in the sources linked here. Last reviewed April 2026.
Educational only. Nothing here replaces a conversation with your healthcare provider.